Cleft Palate and Lip: Causes, Treatment and Speech Therapy
In This Article Fun Speech Therapy At-home Practice with Speech Blubs How Common Are Cleft Palates and Lips? Cleft Palate Causes and Risk Factors Cleft Palate Treatment Speech Therapy for Cleft Palate
 By Stacie Bennett•Jan 21, 2022•6 min.
By Stacie Bennett•Jan 21, 2022•6 min.
In This Article
- Fun Speech Therapy At-home Practice with Speech Blubs
- How Common Are Cleft Palates and Lips?
- Cleft Palate Causes and Risk Factors
- Cleft Palate Treatment
- Speech Therapy for Cleft Palate
Clefts are described based on the structures involved (lip, alveolus, hard palate, soft palate), laterality (unilateral left, unilateral right, or bilateral), and severity (width and extent of structures involved). Clefts can be isolated (cleft lip only or cleft palate only), or they can occur in combination. They can be unilateral (one sided) or bilateral (both sides), and they can be complete or incomplete (ASHA).
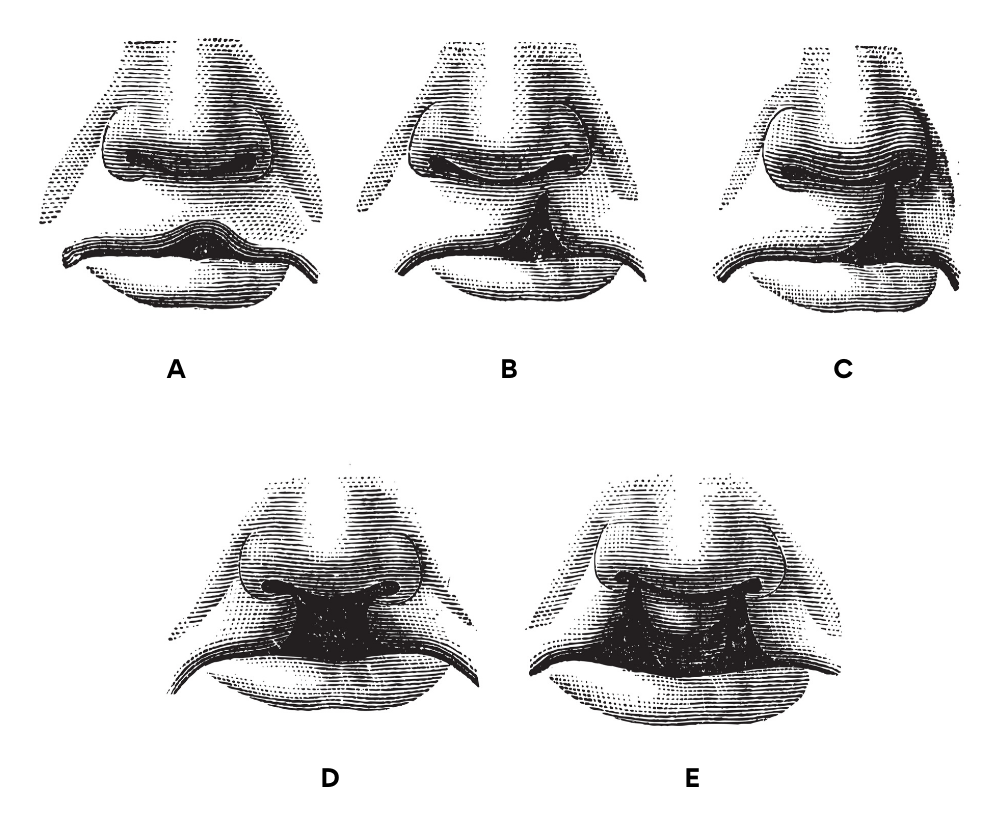
The above image shows the different types of clefts that can occur. They range in depth, severity and location. Pictures (d) and (e) are the most severe forms of cleft palate.
Cleft lip and cleft palate can be associated with a large number of craniofacial and genetic sequences or syndromes, some of which are rare.
Some examples include the following:
- 22q11.2 deletion syndrome (a.k.a. velocardiofacial syndrome [VCFS] and DiGeorge sequence)
- Stickler syndrome
- Pierre Robin sequence
- Van der Woude syndrome
- Treacher-Collins syndrome
- Craniofacial microsomia (spectrum of disorders, including Goldenhar syndrome)
- Neonatal Abstinence Syndrome (NAS), which includes Fetal Alcohol Spectrum Disorder (FASD)
Fun Speech Therapy At-home Practice with Speech Blubs
The more you practice, the more you learn! Try Speech Blubs app for fun and engaging therapy sessions with your little one.

How Common Are Cleft Palates and Lips?
Worldwide, oral clefts in any form (i.e., cleft lip, cleft lip and palate, or isolated cleft palate) occur in about one in every 700 live births (World Health Organization [WHO], 2001).
International estimates that are limited to cleft lip with or without cleft palate range from 7.94 to 9.92 per 10,000 live births (IPDTOC, 2011; Tanaka, Mahabir, Jupiter, & Menezes, 2012).
Cleft lip, with or without cleft palate, is the second most common birth defect in the United States, affecting one in every 940 births and resulting in 4,437 cases every year (Parker et al., 2010).
Cleft Palate Causes and Risk Factors
There is no one cause of cleft lip and palate. However, most cases are thought to result from multifactorial inheritance — an interaction between the person's genes (genetic predisposition) and specific environmental factors (see, e.g., Beaty et al., 2011). Clefting can also be caused by chromosomal differences in individuals born with genetic syndromes.
Risk factors that increase the likelihood of cleft lip and palate include the following:
- Strong family history of cleft lip and palate (e.g., Grosen et al., 2010; Natsume, Kawai, Ogi, & Yoshida, 2000; Sivertsen et al., 2008).
- Race—cleft lip and palate are more common in Asians and Native Americans than in African Americans (see Incidence and Prevalence section).
- Sex—males are more likely to have cleft lip with or without cleft palate; females are more likely to have cleft palate without cleft lip.
- Exposure to certain environmental substances, such as tobacco and alcohol, prescription drugs, and illegal drugs (e.g., Arpino et al., 2000; DeRoo, Wilcox, Drevon, & Lie, 2008; Källén, 2003; Li et al., 2010; Little, Cardy, & Munger, 2004; van Gelder, Reefhuis, Caton, & Werler, 2009).
Cleft Palate Treatment
Treatment for any craniofacial abnormality will include a wide range of professionals. These people will include, nurses, doctors, speech pathologists and patient care coordinator. Treatment may also include early feeding intervention, dental care and orthodontics, audiologic care and monitoring of hearing status, and psychological services.

Treatment may also require surgery to fix the cleft. If surgery does not occur, the child will present with articulation and phonological deficits, issues with the nasality of their speech and dental issues.
Surgery typically occurs within the first 6 months of life for cleft lip repair and within the first 12 months of life for cleft palate (ASHA).
Speech Therapy for Cleft Palate
An integral part of your child’s team will be a speech-language pathologist (SLP). This person will work on the following items:
- Using phonetic placement techniques, typically starting with bilabials (sounds such as /b/ /p/ and /m/ and then moving to progressively harder sounds.
- Introducing gentle whispering or using sustained /h/ to teach easy oral airflow.
- Inserting /h/ after oral stop consonants to discourage use of glottal stops prior to vowel onset [e.g., p(h)op for "pop"].
- Teaching your child to discriminate between sounds that are produced correctly or incorrectly. Self-monitoring will be important for when they are discharged from therapy.
- Providing visual cues, including
- using a lateral diagram or a model of the mouth for visual placement cues;
- pointing to lips/tongue to cue placement;
- using visual airflow cues (e.g., using a feather and having your child blow air out of their mouth to watch it move); and
- using mirrors for observing articulatory positioning (where is their tongue when producing the /l/ sound)—sit side-by-side, so that the child can view the reflection of themselves and the therapist for modeling purposes.
- Providing verbal cues such as instructions for correct placement and manner or airstream.
- Providing tactile (touch) cues, such as
- feeling one's neck musculature to help identify incorrect placement for glottal stops (/k/ and /g/ sounds)
- feeling a released puff of air on one's hand during the production of sounds such as /p/;
- using one's finger to feel their lips close and oral air pressure on sounds such as /p, b m/; and
- using nose plugging/pinching (nasal occlusion) to provide the individual with the sensation of oral pressure and to discourage nasal airflow errors (ASHA).
Another goal that a speech pathologist might work on is feeding and swallowing issues. A baby born with a severe cleft will need to get their nutrition in a modified manner. This might mean making modifications to their feeding position or giving them a different type of bottle. The speech therapist and lactation consultant will work on introducing solids and liquids to your baby in a safe and timely manner.
One of the most important items to remember with feeding is to keep it as low stress as possible for the baby AND the parents.
https://www.youtube.com/watch?v=-xUGpcOslsM
Bottle-Feeding Your Baby with Cleft Lip/Palate
About the author